 The cost of employing a live-in aide can range from roughly $175 to more than $300 per day, depending on the agency and the clients’ needs. But for several of our clients, the out-of-pocket expense is substantially lower because they have so-called long-term care (LTC) insurance.
LTC policies make perfect sense when you consider round-the-clock home care can cost more than $100,000 annually, and a private room in a nursing home can be twice as much. There are tax advantages as well, since the premiums are partially deductible as medical expenses. But as thousands of older Americans have discovered, the cost of maintaining an LTC policy has risen dramatically in the past few years. The headline of a recent New York Times article says it all: “Your Long-Term Care Insurance Spiked. Now What?” The Times cites the example of Karen Herzog, a retired school teacher who received notice from her insurance carrier that her monthly premium was set to double to $550. “Many of us will be forced to drop this policy,” Herzog told the Times’ personal-finance reporter, Tara Siegel Bernard. “This was supposed to be my parachute.” Long-term care policies are designed to cover some or all of the cost of a home-care aide when the policyholder no longer can perform at least two “activities of daily living,” including feeding, bathing, dressing and toileting. Studies show that half of all Americans now turning 65 will require long-term care at some point. Most will need assistance for less than two years, but one in seven will need it for more than five years, according to the Times. That fact helps explain why insurers have aggressively hiked premiums for LTC policies. But there’s more. “Why are premiums swelling so much? There are several factors, but two of the more serious problems involved the predictions insurers made roughly two decades ago. Not only did they underestimate how long policyholders would live, they overestimated how many people would drop their policies, [in which case] insurers would not have to pay claims.” Many insurers -- including the biggest provider of LTC policies, Genworth -- ran into financial trouble. Genworth has agreed to sell itself to a Chinese company, though a deal has yet to be finalized. There are now only a dozen or so insurers offering LTC coverage, down from more than 100 at the market’s peak. Those that are left have petitioned state insurance regulators to increase premiums for tens of thousands of customers. “There is an inherent tension as a regulator,” Virginia’s insurance commissioner told the Times. “You want to protect consumers against rate hikes, but you also want to make sure the carriers remain solvent and are able to pay claims in the future.” Meanwhile, rate hikes are forcing policyholders like Karen Herzog to make difficult decisions -- including whether to drop their coverage. As a general rule, experts advise the elderly to maintain their coverage if at all financially possible. That’s because even with the premium increases, existing policies are both cheaper and more comprehensive than those being written now. “It’s technically still a deal relative to what coverage costs today,” one expert told the Times. If policyholders no longer can afford to maintain their existing coverage, they have several options. For instance, they could elect to reduce their benefits and/or cut the inflation rate for calculating benefit increases in the future. “You can call and sometimes [the insurer] will be flexible with giving you other options that were not in the package sent in the mail,” said Jesse Slome, executive director of the American Association for Long-Term Care Insurance. For more information, check out my Q&A with Tinton Falls insurance agent Toby Stark, which covers the basics of long-term care insurance. Another good resource is AARP, whose website includes a fact sheet titled “5 Things You Should Know About Long-Term Care Insurance.” Written by T.J. Foderaro
0 Comments
 One of the nicest things about my work at Twin Lights Home Care is getting to know the women who take care of our clients. While they’re all dedicated to helping elderly men and women continue living in the comfort and security of their own homes, some have an inner strength, dignity and sense of duty that’s nothing short of heroic.
A case in point is Cynthia, who started working with our clients earlier this year. So far, Cynthia mostly has performed “relief” duty –- filling in on a case when the regular aide takes time off to spend with her family. While my partner Donna always speaks very highly of Cynthia, I didn’t have a chance to meet her myself until this week, when I picked her up at the Red Bank train station and drove her to the home of a client in Middletown whose regular aide was going off for a week. It’s about a 15 minute ride from Red Bank to the Navesink section of Middletown, so I asked Cynthia a little about herself. I learned that she lives in North Jersey but originally is from Jamaica, as are many of the aides who work with our clients. I also learned she has three grown daughters still living in Jamaica, and several grandchildren. That’s not uncommon: Many home-care workers help support family members in their native countries, often in the Caribbean or the Philippines. I wanted to ask Cynthia how she felt about living apart from her family … but I didn’t. I knew that she had helped care for the client in Navesink once before, so I asked Cynthia how she got along with the woman and her family. “Oh, very good,” she said. “They’re very nice.” I was curious to know how the client, who is in her 80s, was doing both physically and mentally. “Oh, pretty good,” Cynthia said. “She can’t get out of bed, and she’s very tall. And she can’t move her legs, which makes it difficult to clean her.” “That must be challenging,” I said. Cynthia continued: “She can only eat pureed food. Everything has to be finely pureed. It takes her a long time to eat. She sips her food with a straw, but sometimes it can take 15 minutes for her to swallow.” “Wow, that sounds very challenging,” I said. “No, not really,” Cynthia said. “They just need love. That’s all this job is about. Love.” I was speechless for a moment, then continued. “It sure is tough getting old. That’s something my father always used to say.” “No, I want to get old,” Cynthia said. “My family will know how to take care of me. As long as you have love, that’s all that matters.” After I dropped her off, I felt very appreciative for the opportunity to spend a few minutes with a woman who, despite significant personal sacrifice, gives her heart and soul to help the most frail and vulnerable among us –- people she never knew before -– live out their lives in comfort and dignity. When I called Donna to confirm that Cynthia was on the case, I told her about my conversation in the car and asked whether we could use Cynthia in a full-time capacity, rather than for relief. Donna explained that for now, Cynthia would prefer to work part-time. If that ever changes, I would be the first to recommend Cynthia to any client who needs a live-in aide. They would be very lucky to have her. -- Written by T.J. Foderaro  There were times when I was caring for my mother in the final years of her life that I thought I was going to lose my mind. Many times. And quite literally. Although we employed part-time aides to look after my mom at her condominium in Highlands, I was constantly dealing with calls from the building manager, grocery shopping, doctors’ appointments, prescription pick-ups, bills and taxes. As my mother grew frailer in body and mind, there were phone calls at all hours of the day and night. Her door was wide open. She tried to walk out of the building. She was confused. She had fallen. There were days when I felt like I couldn’t go on anymore, had no idea how I’d continue juggling the responsibilities of helping my 82-year-old mother while meeting my obligations at work (two jobs) and home (three children). There were moments when the stress literally made me feel nauseous. I also felt angry, sad, frustrated, guilty. It didn’t occur to me at the time that other people — millions of them — were going through the same thing. “It’s hard,” said Linda Schulman, a New Jersey resident who first cared for her dying husband and then for her elderly mother. “It’s like having a second full-time job. It’s very time-consuming.” Schulman’s testimony is all the more telling because she’s a professional. Her title is director of community relations at Daughters of Israel, a nursing home and rehabilitation facility in West Orange. “It is my day and night,” Schulman said of her work in the nursing home. “I lived it. I breathed it. And then it became my life.” Schulman is among a number of New Jerseyans featured in a lengthy expose that recently appeared in the Asbury Park Press. The series, titled “‘Consuming and Isolating’: Why the Caregiver Crisis Could Strain Public Health Care,” reveals that 1.7 million people in New Jersey — nearly 20% of the men, women and children in the state — “live the life of an unreimbursed caregiver.” “Every day, compassionate Americans devote time, energy and resources to ensure that family members who are disabled, elderly, chronically ill or injured can remain in the stability and comfort of familiar surroundings,” reporter Cheryl Makin wrote. “ These Americans are caregivers -- a growing group who often sacrifice much in their own lives for their loved ones.” Are you a caregiver? If you devote some of your time each week to caring for a spouse, parent or other family member who needs help with “activities of daily living” and/or medical treatment, then you qualify as a caregiver. While there are professional caregivers who get paid for their work, most are family members who are unpaid. A recent study by the United Way found the vast majority of caregivers (86%) are women, mostly between the ages of 50 and 64. Nearly half provide care for a parent. Unlike professionals who work regular schedules, unpaid caregivers can be on call 24/7. Numerous studies show that such responsibility can take a serious toll, both mentally and physically. The United Way study, for example, found caregivers often neglect “their own mental and physical health ailments as they put themselves last in their desire to care for another. Caregivers may feel stress, grief and other difficult emotions while providing care.” It’s no wonder that nearly 20% of caregivers exhibit signs of moderate to severe depression, versus less than 7% of the overall population, according to the United Way. Lucille Deutsch, who runs a geriatric-care agency in Morris County, said many family caregivers “end up more ill than the person they are caring for. They don’t keep their doctors’ appointments, they are not eating right, they are not getting enough sleep, they don’t exercise because they are so focused on caring for this person that they love.” In many cases, family members don’t even realize they’re filling the role of a caregiver, Deutsch added. “I’ve met so many sons and daughters over the years who say, ‘No, I’m not a caregiver, I just go food shopping for my mom and do her laundry or I’ll run to the bank,’” she said. “Those are caregiving activities.” In retrospect, I never thought of myself as a caregiver either. As my mother’s condition worsened, we felt it necessary to hire a live-in aide through an agency. We went through a half-dozen aides before we found someone who was right for my mother. But even then I was often on duty, from stocking my mother’s refrigerator to managing her finances to relieving the aide when she went to church on Sundays. I guess I was a caregiver after all. What can caregivers do to manage the stresses and strains of their “second job”? The Family Caregiver Alliance offers the following tips: 1. Recognize warning signs early. These might include irritability, sleep problems and forgetfulness. Know your own warning signs, and act to make changes. Donʼt wait until you are overwhelmed. 2. Identify sources of stress. Ask yourself, “What is causing stress for me?” Sources of stress might be that you have too much to do, family disagreements, feelings of inadequacy or the inability to say no. 3. Identify what you can and cannot change. Remember, we can only change ourselves; we cannot change another person. Ask yourself, “What do I have some control over? What can I change?” 4. Take action. Taking some action to reduce stress gives us back a sense of control. Stress reducers can be simple activities like walking and other forms of exercise, gardening, meditation and having coffee with a friend. Identify some stress reducers that work for you. 5. Take a break from caregiving. Get help with caregiving tasks either by recruiting other family members or hiring a professional caregiver. Written by T.J. Foderaro  “Her mind was smashed to pieces … but the pieces were still her pieces.”
Thus the narrator of “The Waverly Gallery,” a remarkable play now on Broadway, describes his 85-year-old grandmother as dementia warps her once-brilliant mind beyond recognition. This production of Kenneth Lonergan’s drama, a finalist for the Pulitzer Prize, is a brutally honest look at the effects of dementia both on the one afflicted with the disease and on the family as a whole. It is perhaps the smartest thing ever said on the subject, fiction or nonfiction. In wrapping up his rave review of the play for The Wall Street Journal, drama critic Terry Teachout wrote, “It would be unfair not to warn you going in that if you have any firsthand experience with caregiving, you may find certain parts of ‘The Waverly Gallery’ to be almost unendurably painful to watch.” He’s not kidding. Seeing the play brought back excruciating memories of the years when my mother cared for my father during his battle with Alzheimer’s disease … followed by the period when my sister and I helped care for our mother as dementia ravaged her mind and spirit. Lonergan, whom Teachout calls “America’s greatest living dramatist,” explores the nature and progress of dementia via the character of Gladys Green, a once-prominent lawyer who in her later years opened a small art gallery in Greenwich Village to keep her busy. But now, even the gallery is too much for her to manage, as her family discovers early on in the play. Later, we watch Gladys’ mind unravel during family dinners and other encounters with her daughter, son-in-law and grandson, as well as a young artist whom Gladys invites to hang paintings in her gallery. They struggle to contain their frustration and even anger at Gladys as she constantly repeats herself and makes one mistake after another – for example, giving snacks to the family’s overweight dog despite incessant pleas not to feed him. “It is a harrowingly honest group portrait of the havoc wrought by that disease, not only on those who have it but on those who love them,” Teachout writes. Ben Brantley, reviewing “The Waverly Gallery” for The New York Times, says Lonergan drew on his own experiences watching his grandmother struggle with dementia. The play, Brantley writes, “is a group portrait in which everyday life is distorted to the point of surrealism by the addled soul at its center.” In addition to a powerful script, the production at the John Golden Theater is supported by a brilliant cast, including the great screenwriter, director and comedian Elaine May in the role of Gladys Green. May herself is 86 years old. “Here’s a hell of an acting challenge,” Vinson Cunningham writes in reviewing “The Waverly Gallery” for The New Yorker. He likens the play to “an experiment in speculative neuroscience: What happens when a large personality persists but comes unbound from the structures of memory, custom, and comprehension that once contained it?” Also in the cast is Joan Allen, recognizable from prominent film roles including "The Bourne Supremacy," and Michael Cera, who left an indelible mark in the teenage love story “Juno.” Better than any article or book I’ve read on the subject, the ensemble cast conveys in an immediate and visceral way the emotional and spiritual toll dementia takes on a family. “A family is a finicky machine: when one part starts to falter, the whole thing slows to a halt,” Cunningham smartly observes. “There’s nothing like one member’s slide toward death to send the others spiraling backward and inward – inspecting old arrangements and restarting lapsed arguments, wondering just what it was, besides blood, that ever held them together.” “Spiraling backward and inward” – that’s as good a metaphor as I can imagine for the experience of caring for a loved one who suffers from dementia. Written by T.J. Foderaro  It was the afternoon of New Year’s Eve when my 80-year-old mother called to say she wasn’t feeling well. I knew from the weakness in her voice that I had to get her to a doctor ASAP.
She had been fighting a cough for more than a week. Although I had seen her at Christmas and been calling daily to check in on her, I was shocked when I arrived at her condominium in Highlands. She was slouched on the couch wearing a nightgown that apparently hadn’t been changed for days. She looked pale and drawn, as if she hadn’t been eating or drinking enough fluids. The condo was a mess. The doctor took one look at her and more or less ordered me to take her directly to the emergency room at Riverview Medical Center in Red Bank. That night she was admitted with pneumonia. She remained in the hospital for nearly two weeks. Though it didn’t occur to me at the time, my mother was the victim of what advocates for the elderly call “self-neglect” – a shockingly common occurrence that promises to become even more prevalent as the population of older Americans swells in the coming years. A new report details just how common the problem is. “Across the United States, solitude has become a deadly threat for hundreds of thousands of senior citizens living at home,” according to an exposé published last week by the New England Center for Investigative Reporting. Investigative journalist Paul Singer reviewed data supplied by state adult protective service agencies across the country, including New Jersey. What he found was that last year alone, those agencies intervened in more than 142,000 cases to protect elderly men and women from self-neglect. That’s a huge number. But if anything, the data almost certainly “understates the problem, and probably dramatically,” Singer writes. “The elder abuse data is not complete,” confirms Alice Page, an adult protective service professional in Wisconsin. “It’s correct in terms of what’s reported, but there are so many cases that aren’t reported.” When the media reports on cases of “elder abuse,” it’s typically about some sort of criminal activity. That is, some bad actor – a greedy relative, a drug-addicted neighbor – commits theft or, worse, a violent crime. “But the most common threat,” Singer reports, “is self-neglect: an elderly person unable to provide for their own clothing, shelter, food, medication or other basic needs, and having no one to provide care for them. And it’s a problem that’s growing as the population ages.” Holly Ramsey-Klawsnik, director of research for the National Adult Protective Services Association, said self-neglect accounts for about two-thirds of all cases reported by state agencies nationwide. Until recently, elder abuse in all its forms was a “silent issue,” said Edwin Walker, a senior official at the U.S. Department of Health and Human Services. “For decades, people just didn’t want to address it at all.” Part of the problem is that in a free society, adults are presumed to be autonomous. If they want to stop bathing or cease taking medication, that’s their right. “We talk about the dignity of risk in these cases,” said Alice Paige, the Wisconsin official. “Some people just choose to live with more risk and accept the consequences. And if you give people choices that involve risk, that enhances dignity.” It’s a different matter, of course, when the individual suffers from dementia and is incapable of properly assessing and managing risk. “We do know that self-neglect increases illness, increases emergency room use, increases hospitalization, increases nursing home use, increases hospice use and hastens mortality,” Ramsey-Klawsnik said. That New Year’s Eve when I took my mother to the hospital served as a wake-up call. My sister and I immediately began researching our options, and soon found a home-care agency that placed a live-in aide in my mother’s condo. If you have concerns that an elderly family member no long is capable of taking care of themselves, a good first step is having them evaluated by a physician specializing in geriatric medicine. A doctor can help determine whether any cognitive impairment is temporary -- the result of a small stroke, for example -- or a symptom of a progressive form of dementia such as Alzheimer’s disease. The services geriatric specialists provide was the subject of a previous blog post. Written by T.J. Foderaro  I remember feeling a mix of sadness and anger when the first signs of dementia began to creep into conversations with my mother soon after she turned 80.
She’d say something about all the papers she still had to grade for her journalism students, even though she had stopped teaching five years earlier. Or she’d ask where her dog Kate was, even though Kate had died long ago. Most painful of all was when she’d ask why my father wasn’t home yet – even though it had been 15 years since he passed away. I wasn’t very patient with her – at least not at first. I’d quickly correct her, sometimes angrily. “Mom, you’re not in New York. You’re at Eastpointe, where you’ve lived for almost 10 years.” In retrospect, I could have handled the situation with a great deal more wisdom and sensitivity. Over time, I stopped correcting her, let her go on saying and believing things that were completely untrue. But there was part of me that felt guilty for enabling her to live in a fantasy world. This, after all, was a woman who graduated from Vassar, spent 20 years as an award-winning reporter and editor at the Red Bank Register, then capped off her career teaching journalism at Fairleigh-Dickinson. She was all about logic and facts and intellectual rigor. She was among the deepest thinkers I’ve ever known. I still feel guilty. How to treat someone with Alzheimer’s disease or other form of dementia is among the most challenging issues of our time, raising profound ethical questions with serious implications for all parties involved. I didn’t fully appreciate this fact until I read a remarkable article in the Oct. 8 issue of The New Yorker magazine. (I’m a lifelong reader of The New Yorker because my mother was a lifelong reader of The New Yorker.) The article, by staff writer Larissa MacFarquhar, is titled “The Memory House: Should the Illusions of Dementia Be Corrected or Accepted?” MacFarquhar visited a senior community near Cleveland, Ohio, that not only accepts illusions – it encourages them. “The large central room of the memory-care unit was designed to look like an old-fashioned American town square,” she writes. “There was a small fountain surrounded by plants and a low stone wall; there were a couple of lampposts and benches, tables and chairs set about. … Two long hallways, which led off from the opposite sides of the central room, looked like streets in the same town, with clapboard facades and porches on either side. … The ceiling consisted of bright light panels painted to look like a blue sky dotted with clouds. In the evening, as it began to grow dark outside, lights on the porches came on. Sometime later, the street lamps were lit; and finally, around eight o’clock, the ceiling sky was switched off, so that the unit came to look like a small-town street at night.” What to make of this approach to dementia care? As MacFarquhar discovered, there’s little consensus among experts about whether “simulated presence therapy,” as it’s called, is either effective or moral. Some view it as a “psychological placebo,” while others see it as outright deception tantamount to lying. But is lying to someone suffering from dementia the same as lying to anyone else? “To lie is to violate the respect that one person owes another; but lying to a person with dementia can protect them from awful truths that they have no power to alter,” MacFarquhar observes. “If a woman asks for her husband, having forgotten that he is dead, should you tell her the truth and cause her terrible grief, knowing that this fresh bereavement will likely repeat itself, over and over, day after day? Or should you just tell her that he is at the office? … What is more important, dignity or happiness?” Elder-care experts, it turns out, have been debating the issue for decades. In the 1960s, a doctor-nurse team working with elderly psychiatric patients in the South developed a program called “reality orientation” that was the opposite of “simulated response therapy.” “The core of the program was not giving up hope that even the most bewildered, isolated patient could, with enough training, return to the world,” MacFarquhar explains. The key to the program was facts – constantly reminding patients who they are, where they are, what day it is, etc. “For decades, reality orientation was extraordinarily influential – even now, it is a rare nursing home that does not have a reality-orientation board somewhere on display.” But by the 1980s, some practitioners in the U.S. and U.K. began to reject reality orientation in favor of what one pioneering social worker, Naomi Feil, called “validation therapy.” “She believed that it was wrong to lie outright, but also wrong to correct: the thing to do was to enter into the emotional world of the person with dementia and validate their feelings, because feelings were more important than facts.” Then, in the 1990s, an Englishwoman named Penny Garner went even further in her rejection of the reality-orientation approach. Her first rule: Never contradict anything someone with dementia says. “Garner’s method allowed many people with dementia to avoid panic and misery and to live out their last years in a state of happy delusion,” MacFarquhar writes. “How could that be wrong?” But in fact, Garner’s approach drew strong condemnation from many in the medical community, including the British Alzheimer’s Society. To critics, “even passive lies – artificial worlds and fake bus stops – were just a lazy short-term solution that avoided deeper problems,” MacFarquhar writes of the reaction to Garner’s methods. Ultimately, the debate over how to treat people with dementia touches on deep philosophical questions about the nature of identity -- the essence of being human. Citing the late philosopher Ronald Dworkin, MacFarquhar writes: “When people dread the total dependency of late-stage dementia, they don’t just dread its effect on others; they dread the way it warps the shape and story of their life. For some, the prospect that they might live their last years content with childlike pleasures, kept happy with benevolent lies, would not be a relief but a horror.” Dworkin assumed, however, that the man who dreaded late-stage dementia when he was younger is the “same person” as the elderly gentleman who now seems content with a childlike existence. “But what if the happy [elderly] person can no longer remember anything about the man he once was –- is he still the same person in any meaningful sense? And, if not, is it right to end his happy life in order to preserve the dignity of, in effect, somebody else?” For those of us with family members suffering from dementia, there are no easy answers to these questions –- no black or white, no “right” or “wrong.” But in thinking about them, we inevitably discover something about ourselves. Written by T.J. Foderaro  Caring for an elderly parent, especially one who is physically frail and congitively impaired, is challenging under the best of circumstances. Even with home-care aides to help out, I often felt overwhelmed managing my mother’s finances, grocery deliveries, doctors’ appointments and correspondence -- not to mention weekly chores and home repairs at her condominium in Highalnds.
But in retrospect, I had one very big advantage: my youth. Perhaps the word should be in quotes -- “youth” -- for in fact I was in my early 50s when my mother started to decline. But I was healthy and strong and more or less satisfied both professionally and financially. And my sister, a constant companion in my efforts to help our mom, was similarly situated -- and three years younger. What if it had been otherwise? What if my mother lived another 15 years, at which point I myself would have been a senior citizen? What if I had my own health problems? What if I, too, struggled with memory loss? I was prompted to consider such possibilities by an excellent piece of journalism that appeared last week in the Arizona Daily Star. The lengthy article is topped by an appropriately lengthy headline: “As We Live Longer, More Older Adults Face Caring for Even Older Parents.” It’s not surprising. Since I was born, the average life expectancy in the United States has risen from about 70 to 79. And in healthier, wealthier parts of the country, including Monmouth County, it’s not unusual for men and women to live well into their 90s. According to a recent report from the Center for Retirement Research at Boston College, 12% of children who are caring for elderly parents are themselves 70 or older. At Twin Lights Home Care, about half of our clients are at least 90 years old. More than a few have children in their mid- to late 60s. The Arizona Daily Star spoke to several families in which children in their 60s and 70s are still providing care for their parents. “Caring for frail parents in their 90s and early 100s can be daunting while the caregivers themselves are in their 60s or even 70s,” according to the article. “The situation is forcing older adult children, some of them at or nearing retirement age, to decide if they are physically, mentally and financially capable of caring for a parent at the end of their lives.” The article cites the case of a 100-year-old woman who is cared for by her seven children, ranging in age from 59 to 73. The mother suffers from dementia, has very limited hearing and vision and uses a wheelchair. Imagine the mental, physical and emotional strains that puts on her children. “She would not sleep at night,” said one of her sons, who is 64. “In the day, she would stand at the gate outside yelling for help for 45 minutes. She would try to climb over the fence. It was very stressful.” The situation improved somewhat after a doctor adjusted the woman’s medication. But her children continued to struggle. “We wondered and questioned, could we do this – care for her and keep her safe?” one daughter said. “We relied on each other and learned as we went along.” Although their own retirements have been less than peaceful and relaxing, the sons and daughters of this 100-year-old woman have remarkably positive attitudes. “I find strength in the love I have for her,” a 69-year-old daughter says. “She did so much for me. It is our turn now to do for her. It is not a burden. It is a blessing caring for her.” Written by T.J. Foderaro 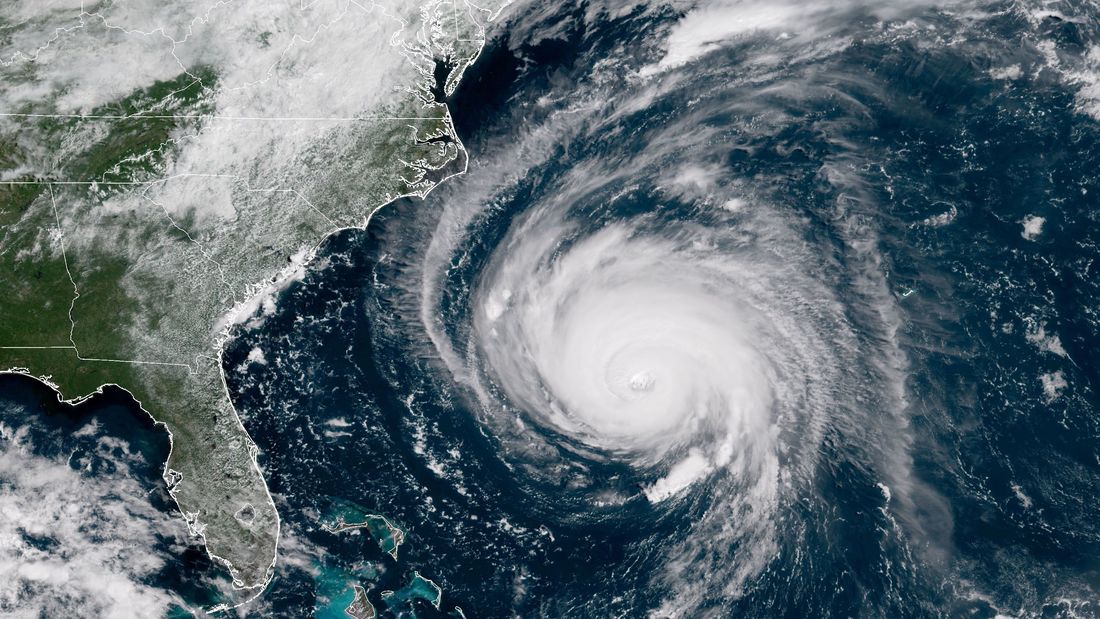 Some of the most dramatic footage of the fury Hurricane Florence unleashed in North Carolina is a video of an elderly woman being airlifted from her flooded home. A Coast Guard rescue swimmer from New Jersey, lowered from a helicopter into the turbulent waters surrounding the house, soon encounters the woman on the front porch. She looks pale and weak.
It turns out the woman had run out of food and medication. “She hasn’t held any food down for at least three days, or water,” Petty Officer 1st Class Steve Maccaferi relays to his crew members, who had flown from Coast Guard Air Station Atlantic City. The video then shows the helicopter lowering a rescue cage and Maccaferi securing the woman inside. She looks scared. But within minutes, she’s receiving the medical attention she needs. The harrowing incident is a reminder that the elderly are particularly vulnerable to severe weather and natural disasters -- and thus require extra support from family, friends and neighbors. Researchers at Brown University’s School of Public Health in Providence, R.I., are using a grant from the National Institutes of Health to study the impact of hurricanes on the elderly. “If there is one thing we have found repeatedly in our research, it is the simple fact that older adults and hurricanes do not mix,” said researchers David Dosa and Kaly Thomas. “Natural disasters such as Hurricane Florence have a profound destabilizing effect on older adults, who have multiple medical problems including functional and cognitive limitations. They often also have medication and nutritional needs that suffer in the days following a storm.” I experienced this firsthand during Superstorm Sandy, which devastated much of the Jersey Shore six years ago. Although I lived only a few miles from my mother’s condominium in Highlands, I was unable to reach her or even talk to her for nearly a week. Then in her late 70s, my mother was beginning to show signs of memory loss and other cognitive impairment. Fortunately, she lived in a building where the residents all chipped in to cook meals on outdoor grills, share flashlight batteries and look after one another. When I finally reached her by cell phone, I learned that she had fared as well as could be expected. Sandy left an indelible mark on the Jersey Shore, and serves as a constant reminder that families need to take special precautions to ensure the safety of older loved-ones during hurricanes, blizzards and other severe weather events. The Brown University researchers emphasize the importance of having a plan in place before a storm knocks out power and telephone service. “If you are a family member living outside of the area, make sure you inquire as to what your loved-one’s plans will be in case cellular phone communication is not possible in the days after the storm,” they say in a Q&A posted on the university’s website. The N.J. Office of Emergency Management offers a “Hurricane Survival Guide” that is loaded with useful information – including tips for people with functional limitations. First and foremost, families need to agree on a communications plan ahead of time. A crucial element of the plan should be to designate a family member or friend who lives outside of the area to serve as a central point of contact. He or she may be able to relay messages and offer reassurances to loved-ones in the storm zone. The “Hurricane Survival Guide” emphasizes the importance of writing the plan down and making copies for the entire family. It also provides a check-list of essential supplies you may need – whether you’re stuck at home or are forced to evacuate. Hurricane kits for the elderly may require additional supplies, such as medications, reading glasses and blood-pressure monitors. “If you or someone close to you has a disability or other access or functional need, you may have to take additional steps to protect yourself and your family,” the Office of Emergency Management advises. Among other things, the OEM recommends registering with local emergency services such as police, first aid squads and fire departments. Churches and nonprofit groups also can provide assistance during emergencies. So far, the 2018 hurricane season has been quiet at the Jersey Shore. But don’t wait until it’s too late to help an elderly family member survive a storm. Written by T.J. Foderaro  The challenge of caring for an elderly parent, especially one with Alzheimer’s disease or other form of dementia, can have a damaging ripple effect on the rest of the family. Inevitably, the burden of daily phone calls, food shopping, doctor’s visits and financial support falls more heavily on some family members than others – typically, those who live closest to the parent. And typically women, studies show.
This can generate serious tension and resentment among siblings that can simmer for months -- or even years -- before exploding in potentially destructive ways. “Of all the difficulties family caregivers face, one of the biggest sources of stress is trying to get on the same page with our siblings,” writes elder-care expert Jody Gastfiend in an Aug. 29 column on Forbes magazine’s website. “While many siblings experience increased closeness caring for their parents, others grow apart.” Gastfriend cites a survey conducted by the Alzheimer’s association that found six out of 10 family caregivers feel they don’t get enough support from their siblings when caring for an elderly parent. Gastfriend’s column – titled “When Siblings Share the Caregiving for an Aging Parent, Will It Be Welfare or Warfare?” -- is a must-read for anyone in this situation. Gastfriend is uniquely qualified to offer advice, having spent years caring for her own parents. She now serves as vice president of senior-care services at Care.com, the leading online marketplace for home-care services. Gastfriend also is the author of an excellent new book titled “My Parent’s Keeper: The Guilt, Grief, Guesswork and Unexpected Gifts of Caregiving” (Yale University Press). In an earlier blog post, I highlighted a chapter of the book that addresses the thorny issue of how to care for aging parents who don’t want help. In her Forbes column, Gastfriend relates the true story of two sisters who suddenly were faced with the challenge of caring for an 89-year-old father who developed Parkinson’s disease. One sister, Kelly, took the initiative to hire a caregiver to help her father with meals, light housekeeping, errands and other essential tasks. But the other sister, Fran, became furious when she learned about the arrangement. Fran felt strongly that her father should be transferred to an assisted-living facility. “It shouldn’t have to be this hard,” Kelly told Gastfriend. “After all, my sister and I both love my father. Why can’t we agree on things?” According to Gastfriend, a common source of conflict among siblings is differing perceptions of a.) how serious a parent’s condition is, and b.) the best way to help. If family members can’t reach a consensus, Gastriend recommends seeking professional guidance from an eldercare manager, also known as an aging life care manager. You can find one through the Aging Life Care Association, which maintains a database searchable by zip code. Another source of conflict is money. Gastfriend cites a recent AARP report that says family members together spend an average of $7,000 per year caring for an elderly parent. “When siblings fight over money, they can lose sight of what is in the best interest of their parents. If disagreements become entrenched, it may be worth reaching out for expert help.” Among those most qualified to offer advice in this area are elder-care attorneys and financial planners. Sibling conflicts can be avoided, or at least mitigated, by holding a family meeting – a topic I addressed in an earlier blog post. The Family Caregiver Alliance offers a comprehensive how-to guide on planning and conducting a family meeting. It’s essential that family members begin communicating early and often, because the stress level will only increase when it comes time to discuss end-of-life care. As Gastfriend observes, “all the forces that pull us apart and hold us together can come roaring to the surface as families face difficult decisions regarding end-of-life care. … Planning ahead can avoid the risk of intractable conflicts that may linger for years –- even generations -- after the death of a parent.” Of course discussing a parent’s impending death is perhaps the most difficult –- and stressful -– conversation siblings will ever face. If you feel you need help in this area, a good resource is The Conversation Project, a website that offers a free “starter kit” to guide siblings in their discussions. Written by T.J. Foderaro  Managing care for an elderly parent can be emotionally draining and logistically exasperating under the best of circumstances. I consider myself lucky because my mother, in her final years, was generally appreciative of the care my sister and I provided either directly or with the help of a series of home-care aides. She had her moments, but for the most part, my mom gladly accepted help. Unfortunately, that’s not always the case with older people grappling with deteriorating health or mental function. Consider the case of Ed, whose health and cognitive abilities went into sharp decline after his wife died. His stepdaughter Jan jumped into the fray, quitting her job to help take care of her father, who suffered from diabetes. “When his blood sugar spiked to a dangerous degree, Ed refused to go to the hospital,” writes Jody Gastfriend in a newly published book, “My Parent’s Keeper: The Guilt, Guesswork and Unexpected Gifts of Caregiving” (Yale University Press). “Jan, upset and alarmed, pleaded with her stepfather and eventually called 911 against his wishes.” Soon, Ed had to have two toes amputated. Then a leg. “Although Ed was able to put on his own prosthetic, he refused to do so and was confined to a wheelchair,” Gastfriend reports. Compounding the challenges for Jan: “Ed would not agree to an outdoor ramp, making movement in and out of the house a Herculean task. He was stuck -- physically and emotionally. And so was Jan.” Gastfriend has accumulated a wealth of knowledge about caring for the elderly based on both her personal and professional experience. She has been a social worker for more than 30 years and currently is vice president for senior care at Care.com, the leading online marketplace for home-care services. In “My Parent’s Keeper,” Gastfriend examines all aspects of caring for an elderly parent, from dealing with difficult siblings to hiring professional caregivers to managing the financial burden. But she’s particularly insightful when it comes to dealing with the parents themselves – especially those who refuse to acknowledge they might need help after a lifetime of helping others. (If you want a sample, Forbes just published an excerpt of the relevant chapters.) “One of the biggest frustrations for adult children is that they come up with a plan that makes perfect sense to them but their parent says, ‘Thanks but no thanks,’” Gastfriend writes. “When our parents’ refusal to accept help puts their safety and well-being in jeopardy, we feel compelled to act, yet our good intentions are often thwarted. I have heard countless stories of caregivers who tried strong-arming their parent to accept help – only to feel angry and dismayed when their efforts failed.” Gastfriend has two simple but wise pieces of advice if you have a parent who clearly needs help but refuses to accept the fact. First, try not to take their rejection personally. It’s not you they’re rejecting, but the notion that they may not be as capable and independent as they once were. And second, try to empathize with their fears and insecurities. Literally, try to imagine being in their place and how you might react under similar circumstances. The exercise can help turn an adversarial process into a partnership. “Offering choices and ceding a little control along the way may help break down the walls of resistance,” Gastfriend observes. Sometimes all it takes is a change of terminology. Gastfriend cites the example of one family who initially had trouble persuading their father to accept help from a professional caregiver. The father, you see, was a retired corporate CEO who was not accustomed to relinquishing control. Wisely, his children stopped using the term “caregiver” and started saying “assistant” instead. That was enough to satisfy their father. If, despite your best efforts, a parent refuses to budge, you may need to seek help from a professional, Gastfriend advises. “Aging life-care professionals, elder-law attorneys and professional mediators can provide an objective perspective about financial and legal matters and lay out options for care. They may also dislodge entrenched parents from unreasonable and unsustainable positions that put them and others at risk.” In an appendix to “My Parent’s Keeper,” Gastfriend distills her experience and insights into three useful tips:
Written by T.J. Foderaro
|
AuthorT.J. Foderaro Archives
February 2020
Categories
All
|
 RSS Feed
RSS Feed
Copyright © 2023, Twin Lights Home Care, All RIghts Reserved